Open vs Closed Rhinoplasty Often...
PROCEDURES:
FACE
BODY
BREAST
MED SPA:





 Dr. Jhonny Salomon has vast experience in different procedures such as Rhinoplasty, Breast Augmentation, Liposuction, Tummy Tuck, Facelift and Eyelid Surgery. He has been featured on Major Television Networks such as The Discovery Health Channel, Telemundo and NBC. You could not be in better hands!
Dr. Jhonny Salomon has vast experience in different procedures such as Rhinoplasty, Breast Augmentation, Liposuction, Tummy Tuck, Facelift and Eyelid Surgery. He has been featured on Major Television Networks such as The Discovery Health Channel, Telemundo and NBC. You could not be in better hands!
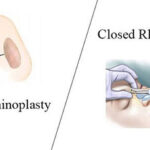
Open vs Closed Rhinoplasty Often...
Chat With Haute Beauty Leaders,...
The Different Types of Rhinoplasty...

Best Age For Facelift A...